Acute Left Ventricular Failure.
Acute left ventricular failure
presents as pulmonary oedema due to increased pressure in the pulmonary
capillaries. But left ventricular failure and pulmonary oedema are not always
synonymous. Acute heart failure may be decompensation of chronic heart failure.
(Anonymous, 2006 )
Causes of Acute LVF
- Acute myocardial infarction or ischemia
- Aortic stenosis or aortic incompetence
- Hypertension
- Mitral incompetence
- Drugs e.g. beta blockers, cocaine
- Infection e.g. Myocarditis.
- Volume overload.
- Anemia.
- Hyperthyroidism.
Signs and symptoms
- Fatigue.
- Pulmonary oedema.
- Dyspnoea - Paroxysmal nocturnal dyspnea.
- Cough.
- Crepitations - after coughing.
- Tachycardia.
- Hypoxia & cyanosis.
- Sweating.
- Cardiomegaly - X ray.
- Dilated pulmonary capillaries and upper lobe diversion - X ray.
- Gallup rhythm - a third heart sound and/or a fourth heart sound.
- Orthopnoea.
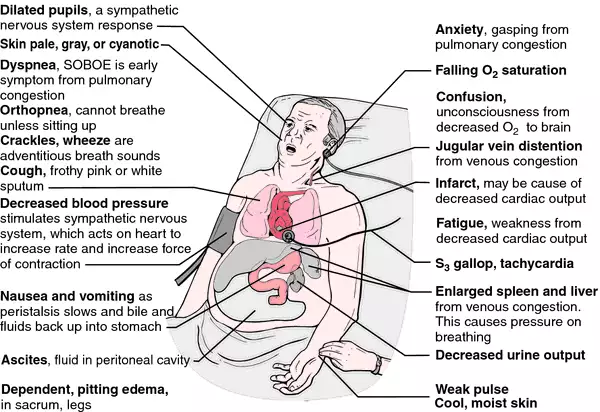
Signs and symptoms of ALVF
( http://img2.tfd.com/mk/H/X2604-H-14.png )
Investigations
1. ECG
2. Echo cardiograph - The echo cardiograph is the most frequently used investigation. Echo cardiography is the key test to
provide a semi-objective assessment of cardiac function. It enables an
assessment of:
Overall
LV systolic function
Diastolic
function
LV
wall thickness
Valvular
diseases.
Estimation
of pulmonary artery systolic pressure.
3. Serum
natriuretic peptides (B‑type
natriuretic peptide [BNP] - - If Acute LVF BNP is more than 100 mg/liter.
4. N‑terminal pro‑B‑type
natriuretic peptide [NT‑proBNP] – If acute LVF NT‑proBNP is more than 300 mg/liter.
( In people presenting with new
suspected acute heart failure with raised natriuretic peptide levels, perform trans thoracic Doppler 2D echo cardiography to establish the presence or absence
of cardiac abnormalities. ) (NICE guidelines, 2014)
5. Blood tests - FBC, U&E and
creatinine, glucose, fasting lipids, thyroid function test
.
6. CXR – Chest X Ray provides details
of
Cardiomegaly (cardio thoracic ratio
>50%)
Ventricular
hypertrophy
Peribronchial cuffing.
Fluid
in the fissures
Pleural
effusions

CXR - ( http://upload.wikimedia.org/wikipedia/commons/1/1c/PulmEdema.PNG )
7. Urinalysis.
8. Lung function tests (peak flow or
spirometry).
9. Cardiac magnetic resonance imaging
- For assessing ventricular volumes, mass and wall motion. It can be used with
contrast to identify inflammation, infiltration and scarring of the myocardium.
( (Kavanagh, 2012).
Management
Initial Management
The patient should be sitting upright and assessed by the ABC
approach.
A - Check the patient’s airway and
administer high flow oxygen through a reservoir bag (also known as trauma
mask).
B - Monitor
the patient’s breathing and look for evidence of fatigue (if concerns then an
urgent anesthetic/ICU opinion should be sought). Pulse oximetry should be
used.
C - Assess the patient’s
circulation by measuring pulse and blood pressure and feeling their peripheries
to check perfusion. The patient should be on a cardiac monitor to identify any arrhythmia s. Insert an intravenous cannula.
Immediate management
Morphine IV as required – this will
help allay the terror and anxiety but may also reduce preload and after load Oxygen.
Drug therapy
- Intravenous diuretic (frusemide), venodilator (isosorbide dinitrate), arteriolar dilator (hydralazine), and positive inotropic stimulation (prenalterol) as first-line therapy for acute left ventricular failure.
- Second line treatments include dobutamine, especially if the systolic blood
pressure is below l00mmHg. Bronchodilators such as beta -2 agonists or
aminophylline may be used if wheezing is present - 'cardiac asthma'.
1. Diuretics: help by reducing circulatory volume and thereby
reducing preload. An intravenous loop diuretic such as Frusemide is
administered in the first instance (Frusemide).
2. Venodilators: an intravenous infusion of Glceryl Trinitrate
may be useful in reducing preload and after load and may also improve coronary
blood flow.
3. Inotropic drugs: these drugs are used to increase myocardial
contractility and output. They are often classified according to their activity
at alpha and beta receptors.
4. Dobutamine : Exerts its
effects on beta 1 and beta 2 receptors and thereby Increases myocardial
contractility and output.
5. Dopamine : Exerts its effects on dopaminergic, beta 1 and beta 2 receptors. At low dose (0.5 - 2 mcgs/Kg/min) it has mainly dopaminergic
effects ~ increased renal blood flow and diuresis.
6. ACE Inhibitors : ACE inhibitors have been shown to reduce
symptoms and signs of heart failure, and improve exercise capacity. Renal
function and serum potassium must be monitored before initiation.
7. Spironolactone : Patients
with severe heart failure and left ventricular systolic dysfunction should be
treated with low dose spironolactone (25mg ) unless there are contra
indications. Monitoring of serum potassium is mandatory.

Management of ALVF
( http://eurheartj.oxfordjournals.org/content/ehj/29/19/2388/F7.large.jpg)
Non-pharmacological interventions
1. Diet
Salt - Dietary salt should be reduced as much as possible by
avoiding the intake of salt rich foods.
Fluid
intake - Excessive fluid intake
should be avoided.
Obesity - Obesity should be reduced. Patients should be advised about
setting realistic targets to reduce body weight. This will require counselling
about behaviour change as well as nutritional advise.
2. Alcohol - Alcohol should be avoided completely in patients with alcohol
induced cardiomyopathy. In other patients with heart failure, alcohol can be
consumed in small amounts.
3. Smoking - Patients should be advised to stop
smoking and their readiness to do so assessed.
4. Exercise - Appropriate exercise is beneficial
for patients with stable heart failure and structured programmes for patients
with heart failure, including long term maintenance, are to be developed in the
future.
REFERENCES
- Anonymous. (2006 , august 14). Acute Left Ventricular Failure (LVF). Retrieved April 28, 2015, from www.skills4nurses.com: http://www.skills4nurses.com/index.cgi?article+146
- Anonymous. (2013). acute left ventricular failure. Retrieved April 28, 2015, from www.gpnotebook.co.uk: http://www.gpnotebook.co.uk/simplepage.cfm?ID=-778436541
- Kavanagh, S. (2012, 07 29). Heart Failure Diagnosis and Investigation. Retrieved 04 28, 2015, from http://www.patient.co.uk/: http://www.patient.co.uk/doctor/heart-failure-diagnosis-and-investigation
- Verma SP, Silke B, Hussain M, Nelson GI, Reynolds GW, Richmond A, Taylor SH. (1987, July 10). First-line treatment of left ventricular failure complicating acute myocardial infarction: a randomised evaluation of immediate effects of diuretic, venodilator, arteriodilator, and positive inotropic drugs on left ventricular function. Retrieved april 28, 2015, from pubmed: http://www.ncbi.nlm.nih.gov/pubmed/2441152
No comments:
Post a Comment